Post POT-KISS-POT FFR Measurements For A Multi-vessels Disease Patient
By: Prof. Emanuele Barbato

Today, interventional cardiologists are increasingly treating patients with complex diseases. To achieve physiologically successful revascularizaiton, physicians have gradually adopted post-PCI assessement. The TruePhysio® pressure microcatheter is excellent in maintaining the wire position while being pulled back, either pre- or post-PCI. Below case operated by Prof. Barbato highlights how the TruePhysio® pressure microatheter facilitates physiological assessment for a patient with multi-vessel and bifurcation disease pre- and post-PCI.
Patient history
72-year-old female
Multi-vessel disease
Risk factors: Type II Diabetes Mellitus, Dyslipidemia and Obesity (BMI 35.2)
Due to inferior STEMI, the primary PCI to RCA (DES 3mm x 23mm) was performed in Dec. 2012
Case challenges
Bifurcation (LAD-D1),
Multi-vessel disease (LAD, LCX)
Side branch physiological assessment by crossing the stent struts
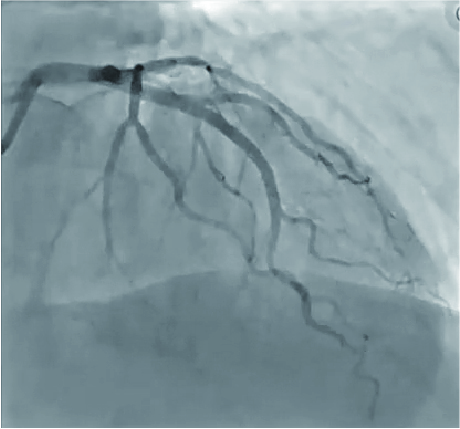
Coronary angiography






Coronary angiography
This case highlights:
The necessity to have microcatheter-based physiology techniques in the Cath Lab which allows physicians to measure FFR values after stent placement
The TruePhysio® pressure microcatheter facilitated the operator to evaluate the function of the side branch after the POT-Kiss-POT technique
The ease of use of the TruePhysio® pressure microcatheter in physiology assessments
LCX and OM1 Lesion
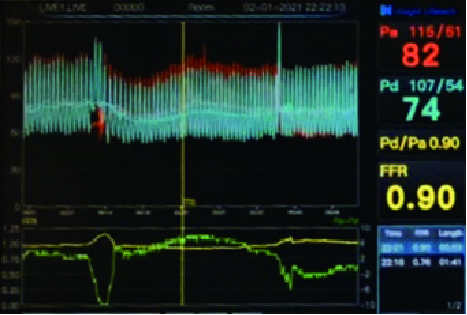
TruePhysio® pressure microcatheter was delivered in the LCX distal to the lesion. After papaverine injection, FFR = 0.90 (Fig. 1)
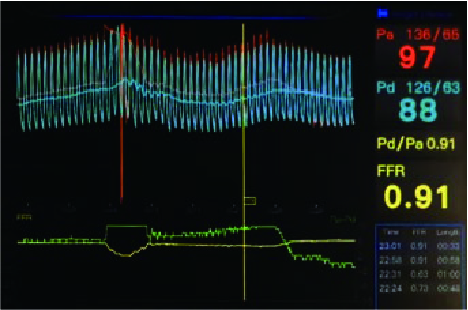
The same workhorse wire was pulled back from the LCX, then navigated to distal OM1, without much effort
TruePhysio® pressure microcatheter followed the above workhorse wire and measured OM1 FFR as 0.91 (Fig. 2)


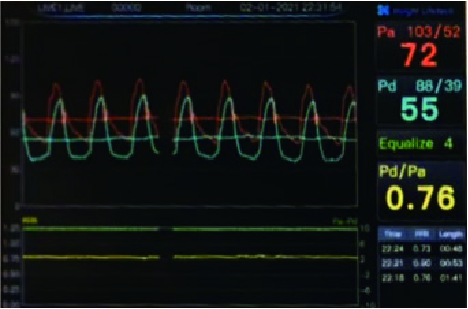
LAD and D1 Bifurcation Lesion
After delivering to the distal LAD and acquiring an FFR value of 0.76 (Fig. 3), TruePhysio® pressure microcatheter was pulled back for discerning the most severe lesion. Intervention to this lesion was decided
Predilating the lesion using a 2.5 x 15mm semi-compliant balloon then an everolimus-eluting stent was placed
Using a 3.0 x 12mm non-compliant balloon for proximal optimization technique (POT)
After wire exchange, kissing was performed with 2 semi-compliant balloons (3.0 × 15 mm placed in LAD and 2.0 × 15 mm placed in D1)
Final POT was performed with a 3.0 × 12 mm NC balloon
Post-PCI FFR for distal LAD was 0.93 (Fig. 4), indicating the ischemia was relived
Pullback assessment showed the residual disease in LAD were diffuse, which would be benefited more by medical treatment.
TruePhysio® pressure microcatheter was advanced to the distal D1 without any effort and given an FFR value of 0.90 (Fig. 5), with satisfactory angiographic results (Fig. 6)




Summary
The TruePhysio® pressure microcatheter could be conveniently delivered to the desired position.
Microcatheter-based FFR measurement takes <1 minute.
No need to rewire for post-PCI measurements.
The TruePhysio® pressure microcatheter can advance directly to the landing zone and the physician only need to administer contrast media while positioning the guidewire.
PHYSICIAN COMMENTS
This microcatheter based FFR measurement system introduces a significant degree of simplification in our invasive functional assessment which is a major step forward in our daily practice.
With a traditional pressure wire I would never performed a FFR measurement of the diagonal branch after a POT-Kiss-POT procedure.
It is astonishing to perform a satisfactory functional physiology evaluation in such a short time frame.