Excellent Deliverability in A Tortuous Vessel with An Acute Angle
By: Prof. Salvatore Brugaletta

The presence of severe vessel tortuosity and angulated lesions have long been recognized as significant predictors of PCI failure 1. Due to increased lesion complexity, coronary tortuosity can lead to difficult arterial wiring delivery during angioplasty, resulting in a reduction in successful PCIs and worse clinical outcomes 2. With superior flexibility and crossability, the TruePhysio® pressure microcatheter can be delivered to the distal of the lesion in tortuous vessels over the workhorse wire 3. This case highlights the need for a pressure microcatheter that can be used in severe tortuous vessels.
Patient History
65-year-old female
NSTEMI and treated with a stent implantation in the right coronary artery (RCA) in 2008
Admitted for unstable angina in 2019.
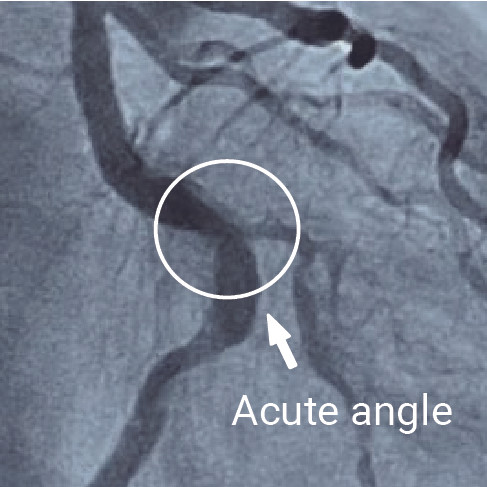
Angiography showed a moderate stenosis (50 - 60%) of the left circumflex artery (LCX) with tortuosity (Fig. 1, 2)
Risk factors: Diabetes, Hypertension



Case Challenges
Difficulty in delivering the interventional device and the increased risk of vessel dissection and vessel perforation
Techniques Used
Pre-PCI and post-PCI FFR with pullback assessment
Pre-dilation and stenting
KEY LEARNINGS
This case highlights:
The necessity to have physiologic techniques with exceptional deliverability which gives physicians the freedom to measure FFR values in severe tortuous vessels
The excellent flexibility and pushability of the TruePhysio® pressure microcatheter
Procedure
A workhorse wire was used at the beginning but it did not cross the lesion because it got stuck.
Then another 0.014″ guidewire was selected and it crossed the lesion in seconds.
The TruePhysio® pressure microcatheter was advanced over the wire and it crossed the lesion easily.
FFR measurement was performed after the injection of adenosine and it showed a value of 0.68 (Fig. 3), meaning that this lesion was significantly important.
A 3.5 mm × 13 mm NC balloon was used for the pre-dilatation of the lesion and then a 3.5 mm × 13 mm stent was implanted.
Post-PCI FFR measurement with pullback assessment was performed after stenting, and the final angiogram showed the reduction of stenosis (Fig. 4).




Summary
The physiology assessment in tortuous vessel can be challenging due to the fact that pressure wire usually has a lack of torque ability.
Microcatheter-based FFR allows the use of your workhorse wire in challenging cases.
PHYSICIAN COMMENTS
In our Cath Lab, we have three different options to measure FFR, the other two are wire-based. Specifically looking at the characteristics of this angled artery, considering the well-known low navigability of a pressure wire, we saw that the TruePhysio® pressure microcatheter was the best option because we were able to use our workhorse wire and placed the microcatheter over it.
TruePhysio® pressure microcatheter could easily pass the anatomy with an acute angle only in seconds which would take a pressure wire to perform in 10-15 minutes.
The pullback and post-PCI measurements were performed very easily and quickly.