Case Study Exceptional Crossability In Heavily Calcified Lesions
By: Dr. Krzysztof Pujdak

The correlation between angiographic stenosis and hemodynamic significance has been proved to be poor in patients with heavily calcified coronary lesions and FFR measurement is needed to interrogate intermediate lesions 1. As one of the most challenging lesions to treat, moderate-to-severe coronary calcification is encountered in up to one-third of coronary lesions 2. With a rapid exchange design and an ultra-thin profile, the TruePhysio® pressure microcatheter can be delivered to the distal end of calcified lesions over the workhorse wire 3. This case highlights the need for a pressure microcatheter that can be used in quite challenging anatomy with tortuous and heavily calcified circumflex artery and a long stenosis of unclear hemodynamic significance.
patient history
77-year-old male
Multivessel disease
Chest pain for several weeks and dyspnea NYHA II
Echo revealed hypokinesia of posterior and interior wall with an ejection fraction of 40%
Risk factors: Dyslipidemia, Hypertension, Chronic Obstructive Pulmonary Disease and Insulin-Dependent Diabetes Mellitus
Baseline angiography showed 80% stenosis and calcification of the mid-left circumflex branch (LCX) (Fig. 1-2)


Case Challenges
It may be challenging to advance the pressure wire/microcatheter to the distal of the heavily calcified lesions.
Techniques used
Rotational atherectomy
Stenting
Pre-PCI and post-PCI FFR measurements with pullback assessment
Key learnings
The case highlights:
The necessity to have physiologic techniques with exceptional crossability that allows physicians to measure FFR values in heavily calcified lesions.
The ease of use of the TruePhysio® pressure microcatheter in physiological assessments.
Procedure
A 0.014″ guidewire was delivered to the distal LCX.
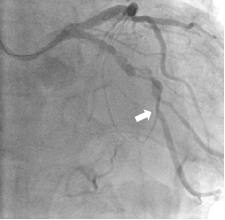
A TruePhysio® pressure microcatheter was advanced in the LCX but could not go any further due to severe stenosis and calcification. The location it reached is shown by the arrow in Fig. 3.
The resting Pd/Pa was 0.64 in this location.
A balloon catheter was selected for pre-dilation, while it turned out that the balloon catheter could not go any further than the location shown in Fig. 4.
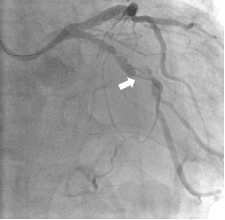
The TruePhysio® pressure microcatheter showed a higher crossability than the balloon catheter, which is specifically engineered for crossing the most difficult lesions and tracking anatomy.
Given the resting Pd/Pa value of 0.64 in the LCX lesion without the administration of adenosine, this lesion was considered clinically significant by the physician, and the PCI strategy was selected.
The guidewire was changed to a rota wire over a support single-lumen microcatheter.
Rotational atherectomy was performed with a 1.5 mm bladed rota balloon.
After multiple pre-dilatations, two DES were placed in the lesion of LCX.
The TruePhysio ® pressure microcatheter was delivered to the distal LCX. After the injection of adenosine, the FFR value was 0.96 (Fig. 5).
The final angiogram showed the reduction of stenosis (Fig. 6).
The pullback assessment was performed and no significant gradient appeared, which indicates the absence of residual ischemia.
Summary
Microcatheter-based FFR can be a good solution to overcome the challenges in complex anatomy.
Rechecking the FFR measurement after the completion of PCI is a reliable confirmation of favorable stent deployment.
Rechecking the FFR measurement in complex lesions where the device (balloon, stent, etc.) is advanced over specialty wires is much faster with a microcatheter-based technology
Physician comments
In this case, the conventional pressure wire wouldn’t go down to the distal LCX and we wouldn’t do that. While for the TruePhysio® pressure microcatheter, it is not a big problem.
With TruePhysio® pressure microcatheter, there is no need to advance the wire once again for rechecking FFR after stent implantation, it is really a nice device to have.
1 Paul M. Johnson, et al. Angiographic severity does not correlate with fractional flow reserve in heavily calcified coronary arteries. Catheter Cardiovasc Interv. 2016
2 Alexander G Truesdell, et al. Calcified Lesion Assessment and Intervention in Complex Percutaneous Coronary Intervention: Overview of Angioplasty, Atherectomy, and Lithotripsy. US Cardiology Review. 2020
3 Chenguang Li, et al. Multicenter clinical evaluation of a piezoresistive-MEMS-sensor rapid-exchange pressure microcatheter system for fractional flow reserve measurement. Catheter Cardiovasc Interv. 2021